Are Medical Scribes the Best Option to Combat Physician Burnout?
By: Steve Moberg
Chief Operating Officer at Team Care Medicine, LLC
In the on-going battle to combat physician burnout, many hospital administrators and / or physician group leaders desiring to help, face the dilemma of adding yet more costs to an operation likely already struggling to turn a profit. In other cases, when administration is not providing the help, many exasperated doctors are paying for a scribe out of their own pocket.
The burnout issue is real and hiring a scribe to help with the heavy EHR documentation burden is becoming a common approach to solving it. A few years ago, the College of Medical Scribe Specialists predicted 100,000 scribes would be employed by 2020. With the Covid Pandemic, it is hard to tell exactly where the number stands today but the bottom line is it is a fast-growing solution. At about $15 per hour (a rough national average ) the annual expense with benefits can reach $25,000 to $35,000. So desperate is the situation, they add this expense with no guarantees of financial returns sufficient to pay for it. Yes, a scribe will bring some relief from EHR documentation, but the resulting productivity gains are mixed. Some doctors see a 6%-8% (the high end of the range) productivity lift, however, a 2019 $480,000 scribe model pilot at St. Charles Medical Group in Bend, Oregon was scrapped because the “modest” productivity gains (only ½ a patient visit added per day) were insufficient to pay for the scribes. For about the same cost, administrators could upgrade to a more powerful solution that has been proven to boost physician productivity by 20%-40% or higher. That kind of productivity gain will easily pay for an additional MA being added to the team in lieu of a scribe. In this article, we will compare a Team Care Assistant (usually an MA trained in the use of the Team Care Medicine Model) to the use of a typical medical scribe. We will evaluate what they do and the benefits each provides.
What is a Medical Scribe?
A medical scribe is quite simply a person that interfaces with the Electronic Health Record (EHR) during a patient visit freeing the doctor to focus on the patient. In most situations they require no specific certification or formal training to perform these duties. Candidates that possess soft skills like good listening, good communications, computer (typing) skills as well as some knowledge of human anatomy and medical terminology have an advantage. A high school diploma is a requirement and some background or courses in medicine is a benefit. Typically, a pre-med student is a good candidate however eventually they will move on so turnover may be an issue. A certification program is also available from the American Healthcare Documentation Professionals Group. In most cases, the medical scribe is not in the exam room independent of the physician other than to perhaps room the patient and collect a few vital measurements (temperature, blood pressure, etc.). Lastly, they are not nurses, or even MAs, so there are functions they cannot do which limits their versatility in the practice.
What is a Team Care Medicine TCA?
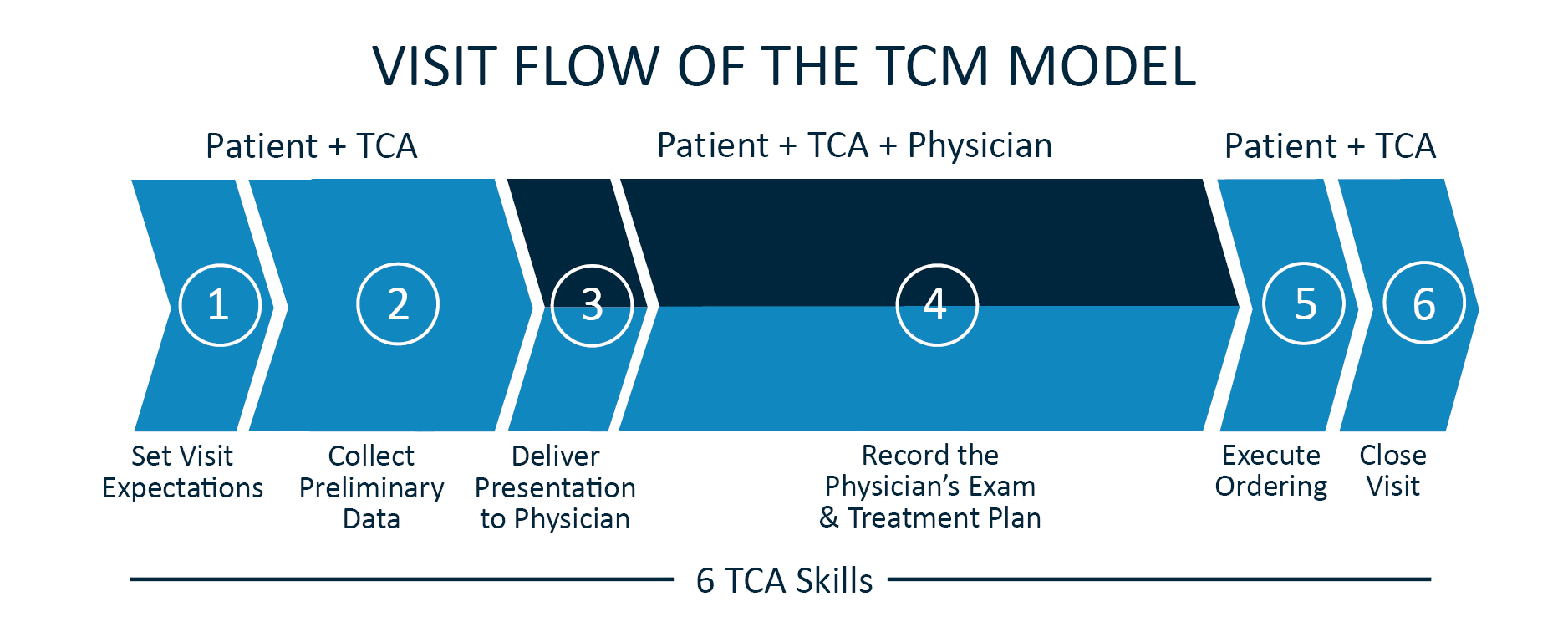
A Team Care Assistant (TCA) is usually a Medical Assistant (MA) or less often a Nurse (LPN or RN) trained by Team Care Medicine to execute a patient visit using the Team Care Medicine Model. The TCA is with the patient throughout the patient visit. They greet the patient and begin their 15-step process (fewer steps for an urgent visit) of interviewing the patient to capture all the patient’s medical information including the use of template driven questions about the chief complaint. Once all the patient’s medical information has been collected and updated in the EHR, the TCA notifies the physician, and the physician enters the exam room. The 5-15 minutes of data collection is then presented in a 2-3 minute crisp, data packed presentation to the physician in front of the patient. After presentation, the TCA then performs the role of a scribe, documenting any additional questions of the provider and answers of the patient. They also document any physical exam findings as well as the diagnosis and treatment plan of the physician in the EHR. Once the doctor has completed explaining the treatment plan to the patient, the doctor is free to exit the exam room and leave the TCA to again go over the treatment plan, perform any patient education and close the visit. See the following diagram of the Team Care Medicine visit flow.
How is the TCA Superior to a Medical Scribe?
There are meaningful differences between a scribe and a TCA in the work they perform, the satisfaction they bring to patients and in the superior financial benefit they produce making the TCA a much more valuable addition to the team than a scribe.
Work they perform:
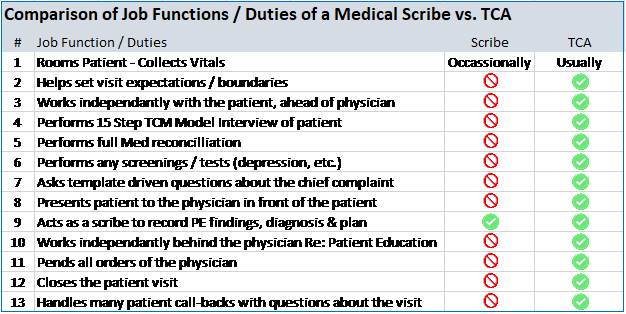
The scribe is generally in the exam room only when the physician is in the exam room. The TCA, as outlined above works independent of the physician during portions of the visit. This is where the significant time savings occurs. A scribe does not collect the patient’s information beyond vitals, nor do they present this data to the physician. A Scribe cannot perform medical procedures or screenings (such as for depression) because they have no medical training. A TCA on the other hand can perform these tasks. A Scribe does not do patient education or review the plan of the provider or close the visit allowing the doctor to slip out sooner, however, a TCA does all these things. A scribe does not take calls from patients with questions about their visit while the TCA fields many of the after-visit patient calls, protecting the physician from work that could easily be done by someone else. A TCA also helps set patient expectations such as helping to keep an urgent visit to just one issue or to let the patient with a list of 10 items know that the doctor will be made aware of them all but may only be able to evaluate 2 today and that an additional appointment(s) may be needed to cover the rest. A scribe does not engage in anything like this. Finally, the TCA working with the physician as a team just gets more done and it is done more efficiently, just like an OR Nurse helps the surgeon inside the operating room. All these differences add up to be significant benefits to the doctors and to the patients throughout the year. The benefits of a scribe are limited because the scope of work they perform is narrower than a TCA’s. See Table-1 For a summary comparison of the differences between a TCA and a Scribe.
The Patient Satisfaction They Deliver
With all the tasks on the plate of a primary care doctor working alone during a patient visit, it is easy for a patient to walk out the door at the end of the visit wondering if the doctor was really listening to them. When they hear the TCA crisply deliver their story to the physician and realize all the data points associated with their care, they know they have been heard. When the doctor explains the treatment plan and then the TCA repeats it and reviews the entire visit, they leave with a better understanding of the plan and what the doctor is asking them to do. Additionally, a 2019 ASHP Survey showed patients are less likely to ask questions about the care plan when they feel the providers are stressed and need to move on. They would more likely ask their questions to the TCA as they feel the TCA is more on their level. When they feel like they truly have a care team looking after them, it is very patient satisfying, and they view it all as better care.
The Financial Benefit They Produce
The TCA is there to significantly increase the efficiency of the physician by doing ALL non-physician work. It takes 2.5 TCAs for a physician to use the Team Care Medicine Model on 100% of the day’s patient visits. Most offices already have 1 to 1.5 clinical assistants per provider. Therefore, usually just 1 additional MA needs to be hired to round out the team. While the doctor and TCA #1 are in Exam Room #1 with Patient #1, TCA #2 is in Exam Room #2 with Patient #2 collecting all their relevant medical information and setting the table for the doctor to enter. When the doctor goes into Exam Room #2 with TCA #2 and Patient #2, TCA #1 wraps up the visit with Patient #1 and then begins the visit for Patient #3. See Diagram-2 depicting the provider hourly workflow.
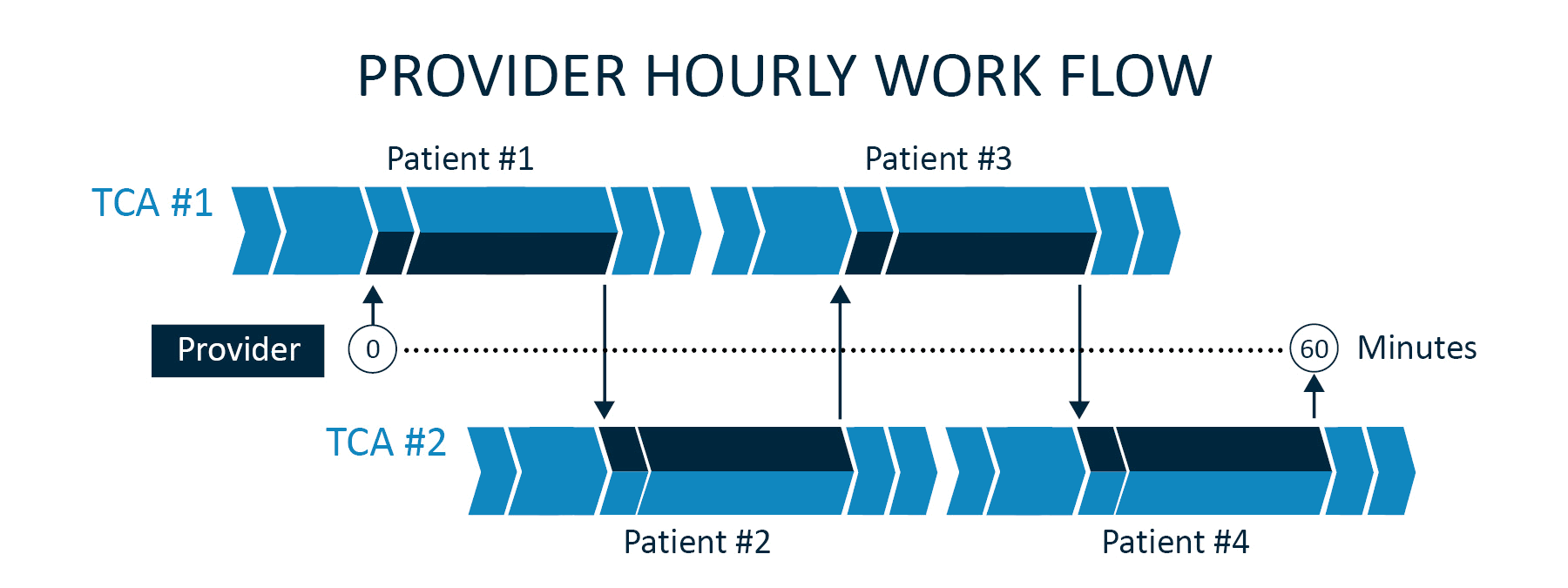
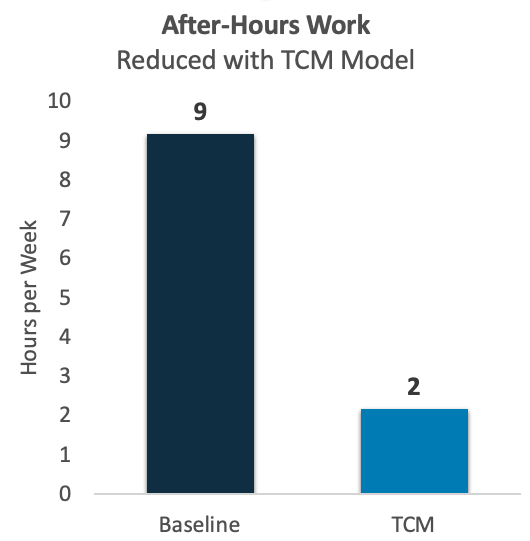
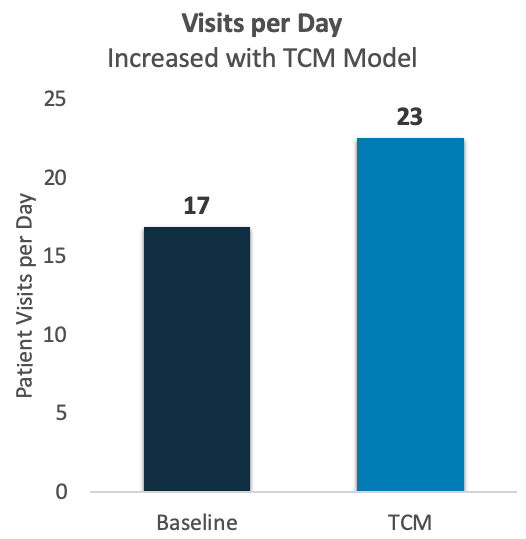
This “dance” is repeated all day with the doctor going from exam room to exam room doing just the work that only they can do. The TCM Model flow also creates natural gaps throughout the day providing doctors a few minutes to knock out an item or two on their task list resulting in less work at the end of the day before heading home. The ability of a TCA to work independent of the doctor produces the big productivity boost over the scribe option. Otherwise, the patient visits are accomplished serially with the doctor and the Scribe doing each together. The TCA typically delivers a 20-40% productivity gain in visit volumes with similar gains in the amount of work they accomplish as a team during the visit (Work RVUs). They help the doctor see more patients and get more done during the patient visit. With similar costs (See Table-2) you get much more bang for your buck with a TCA as opposed to a Scribe (See Table-3).


Conclusion
A Team Care Medicine TCA paired with a motivated doctor looking for a solution to burnout while desiring to maintain the highest level of care for their patients is an overall more powerful and efficient solution than a medical scribe model. Administrators hesitating to add more expense to their primary care offices should have great confidence that they can now add the needed help and that doctors can generate enough additional revenue to more than cover the added expense.